“Perseverence is the hard work you do after you get tired of doing the hard work you already did…“**
Covid – 19 in May 2020
There’s an old expression that people use when describing the attempt to bring change to an organization or group while not disrupting the function of the group, “it’s like building a plane while its in the air”.

In the case of the medical response (we’ll not even get into the national political response) to the COVID – 19 pandemic, we’re trying to build the airplane while its in the air… and its on fire too.
Unfortunately, the medical response has initially been mixed in with the politics and considering that we had nothing to treat this disease at the begining, didn’t harm the response as much as merely confuse the hell out of the general public.
Let’s get to it

What I will do in this post is to review the latest on the drug therapies that we have available and I will separate what is fact-based vs what is my opinion based on what I know and extrapolations.
Hydroxychloroquine
The initial hoopla about this drug comes from early Chinese reports. There were also some communications from France and Italy in which they claimed that there was some decrease in the viral load in the sputum (mucus, spit, phlegm) of people who were given this drug. Why did you give a drug that has no anti-viral properties to these patients? Did the lower viral load improve symptoms? Did the lower viral load improve survival?
The answers (after someone collated and finally looked at the reults) were that 1) they didn’t exactly know why they did it, 2) they were very few of them anyway, 3) the decreased viral load wasn’t significantly (statistically) decreased, and 4) it didn’t seem to improve symptoms nor survival.
So bottom line, it doesn’t work (it never did), it has horrible side effects (including death), and it is a complete waste of time.
Azithromicin
Essentially the innocent bystander in this whole thing, it was used as an adjunct (can something that doesn’t work be used to help another thing that doesn’t work?) to Hydroxychloroquine in the early trial and error phase of Covid treatment. It has an unfortunate side effect of altering the EKG which is usually not a problem as it is given for five days only and usually in relatively healthy people, but in sick patients taking Hydroxychloroquine it was a potentially lethal combination.
Bottom line, it’s good for sinusitis and mild bacterial infection but not COVID.
Convalescent Plasma
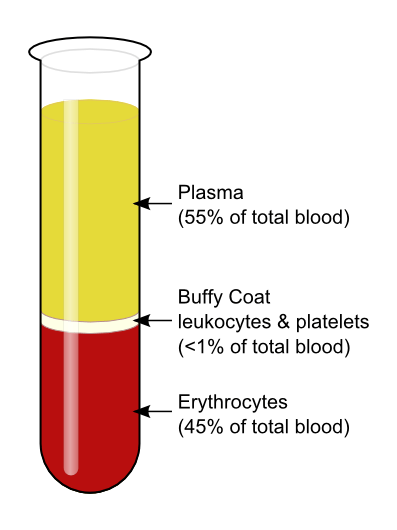
This is an old stand-by of treating a viral type disease that dates back to 1883 when the different components of blood were discovered. The theory goes back even further to the idea of animism, in that the blood of a survivor must have in it the makings of a survivor.
In a more up-to-date sense, we know this to be true as the person who survives a serious infectious disease does indeed make antibodies to that infectious agent. What we don’t know is if these antibodies will shorten the disease, improve symptoms, or improve survival.
It is being given to severely ill patient’s in hospitals. It is intravenous. Plasma is also very tightly controlled and only given by strict criteria. The reason for this is that the blood plasma has many other components such as coagulation factors and such that could in and of themselves be dangerous. It may also be possible to cause allergic reactions in the recipient.
Bottom Line: It is being given. We don’t know when is best, we don’t know the optimal dosage, and we don’t know if it is doing any good. (Opinion: I wish I could say that I saw great improvement in these severely ill patients, but I haven’t). We remain hopeful that this will be an important part of treatment for now. More data to come.
Remdisivir
Originally developed as a broad spectrum (general purpose) anti-viral for Ebola, this drug interferes in the reproduction of the viral mRNA (the chemical that produces more virus) by messing with the mechanisms that hijack the reproducive mechanisms of the host cells. It is not a cure, but it does slow down the replication of the virus, which in turn preserves more of the body’s own native cells, presumably giving the body time to make antibodies.
Bottom Line: It is still strictly controlled. It is intravenous. Since we aren’t really sure when to give it, and how much, we are still sticking to the study criteria that the manufacturers have laid out. In my opinion, this drug would be most useful when given very early in the illness when the virus is first making it’s attack on the body through the lungs. As it is, we don’t have enough drug (as of this writing, there are close to 1.5 million known cases of COVID – 19 in the US alone and if given more than once -protocols are now for twice daily for 5 days – that would be 15 million doses that would be needed tomorrow) to begin to give it to everyone who will eventually need it.
Actemra (Tocilizumab)
Actemra is a member of the class of drugs called a “biologic”. This is used mainly for people with severe arthritis and it comes with it’s own set of side effects which come from its main function as an immune modulator. What this thing does is to block one of the inflammatory chemicals (The “hand grenades” from an earlier post, called IL-6).
Since the really destructive part of the body’s destructive reaction to COVID – 19 is it’s uncontrolled inflammatory response, a drug that can “diffuse the hand grenades” and blunt the out-of-control inflammatory response would help enormously.
The problem is that there are no studies out yet that use this drug in any numbers that would give us good information on how best to give it and for how long.
Bottom Line: We are giving it in the hospitals. It is IV. It is severely in short supply. I have seen some very good anecdotal (personal experience) responses to this.
Synthesis (Opinion)
From here on in I am giving my opinion on treatment. I believe that we must use a multi-pronged approach to this COVID – 19 constellation of symptoms based on how this disease manifests in humans.
When the virus begins attacking the lungs, a Remdisivir type drug should be started to limit the attacking invader. An Actemra type drug should then be used to dampen the massive inflammatory response of the body that causes the actual damage to the tussues (especially distant damage) and then plasma might be useful as an adjucnt to the initial therapy.

Only by using all the tools available to us will be able to temporize and buy time and save lives until a vaccine is created that will help us land the plane (that was on fire) safely.
In future posts I will discuss any changes to the above indications or medications as they come in and out of favor but I won’t rehash any of the older information. Unfortunately, this virus looks to be sticking around for awhile and I don’t want you to get bored.
As always
Wash your hands. Don’t touch your face. Exercise. Eat right. Social distance. Wear a mask in public. Be kind and be patient.
- The opinions expressed here are mine and do not reflect the opinions of any medical organization.
