In the Northeast, the rate of Covid-19 transmission and infection is dropping down to the point where I only have two Covid patients left on my service.
Both of them are relatively young and strong men who will likely need oxygen for the rest of their lives.
Be that as it may, the focus of life as we emerge from isolation, is now on prevention of spread and trying to keep the horror of March / April / May from happening again.
(We all know it’s going to come back in the fall, but for our own sanity, we’re “whistling past the graveyard” and trying to pretend it didn’t happen)
But it did.
I’m Sorry
When I unilaterally declared on a previous blog post that it was over, I was only thinking about it for us… here where I live. Not for the rest of the country.
For that I am sorry.
It isn’t over.
I will not go into politics, but I will go into the discussion of willful ignorance and stupidity.
I would have thought that when the New York area was going through three months of death and upheaval, the rest of the country would have paid attention. When every outlet (official and unofficial) was advising us all on how to stop the spread of this virus, society as a whole would have listened.
Really?
But no.
The medical professionals have listened and are now using the best practices that we developed while we were in hell, to attempt to salvage life. But the populations in the Southeast and Southwest do not honor their healthcare workers, they do not honor their elderly, and most of all do not honor themselves, and do not take measures to protect themselves.
I’m not saying that everyone is doing it, but enough people are blinded by selfish desires couched in the finest rationalizations, to cause spread of Covid and invite death into their midst. The way to stop the spread is well known.
It’s easy.
Grow up, wear a damn mask. Wash your hands. Social distance.
It’s not political, it is human.
In this season of exposed lies, of exposed fear, and exposed hatred… be that spark that exposes love for one another.
In the spaces between seeing patients, calling families, and writing notes come thoughts. Psychologists would call them “invasive”, and yes I know that left unexamined, these things can be dangerous. Luckily, we have our social worker who regularly (and insightfully) does an informal debrief on us.
She probably thinks we don’t notice but we do and we’re thankful.
When did it really start?
The gift shop has St. Patrick’s Day stuff.
When we come into work in the mornings, we are temperature checked and then need to swipe our ID cards into a card reader. What this does, is to document that we’ve been checked and presumably that we are aware of the danger of going to work.
When we were talking about when it really started, an image from this morning came to mind. The card reader is right outside of the Gift Shop. When you look into the gift shop , it’s still full of St. Patrick’s Day cards, green hats, St. Patty Cards, and the very beginning of Easter Chocolate Bunnies.
The gift shop was closed in early March, when all the volunteers were sent home and now sits like a clock frozen at the time of a disaster, it’s cheerful Trinkets heralding holidays that were just days of anxiety and fear in the hospital in which it lives.
The days after that came almost unnoticed, the hours of terror turning us all into zombies, lumbering on under increasingly heavy loads until after two weeks it became normal.
Like Monuments To The Lost
This morning on rounds my team and I had to walk by the security holding closet. This is the closet that hospital security uses to keep an admitted patient’s belongings until they are being discharged or until family comes to retrieve them.
Now normally this isn’t even an after-thought and I’d be hard pressed to even tell you were it is.
I know where it is now.
Like monuments to those lost
Security was emptying the closet of unclaimed bags of personal effects and getting them ready for long-term storage. Hundreds of bags all stacked neatly along the hallway; generic hospital issue clear bags, shopping bags, backpacks with decorative patches, and large inter office envelopes all being labeled with the names of those lost to Covid, awaiting some future relative who would claim them.
As we walked away from that sight, it reminded me of headstones, marking the life of someone who came to us and never left, their lives remembered in a small pile of clothing and shoes.
Images that stoke a memory.
Hope?
Recently, there have been reports of the possible effectiveness of a drug by the name of dexamethasone in treating Covid-19.
Dexamethasone
Dexamethasone is a steroid and what steroids do is suppress the immune response. If you recall, the danger of Covid is the way it stimulates the immune response into destroying the body’s lungs and kidneys. A drug (like Remdisivir and dexamethasone ) that decreases the immune response should help this phase of the disease.
The preliminary reports show that when given at the right time, it improves short term survival by five percent. There is no data about quality of life or long term survival.
So it’s a good thing. Better would be that you wear a mask and don’t get sick in the first place.
I live and work in New York (Long Island specifically) and things have pretty much settled down at our hospitals.
The make-shift ICUs have been dismantled, COVID patients on vents relegated to a small area in the back of the MICU (Medical ICU). The non-intubated people housed in three hallways of the unit that had always been designated for infectious diseases. Those areas still have the COVID look to them, bags taped to walls and blue plastic gowns hung from hooks, but there is less desperation than there was.
The patients that were going to die in the ICUs are slowly dying, regardless of what the families want and what any doctor could ever do. Those not on vents are going home (with oxygen and forever damaged lungs -pulmonary cripples) or still short of breath on high concentration of oxygen and clearly going nowhere.
At least the families can come to the windows and see their relatives from outside the buildings. And we’re beginning to let some families come visit those near death.
Everywhere else in the hospital it’s different. We still all wear masks (a habit that will probably live on for a good long time) but the rooms are now immaculate, the floors shiny and the walls all freshly painted. All hint of the horror covered in bright white with earth-tone trim.
I was rounding with my team this week when our social worker (a brilliant woman who was “parachuted” into the hospital from our hospice affiliate on a grant to help us – she arrived as the “tide” was washing out) noted the look in our eyes and the blank eyes of the nurses on the floors and asked us, “but how did it feel?”
It Was Dark
The lights weren’t bright enough
As a group, including some floor and ICU staff, we all had similar recollections.
It was dark. Not literally, but no matter how many lights were on – the hallways, rooms, and offices felt darker than they should have been. The atmosphere inside was “heavy”, hard to breath.
We all agreed that we actually couldn’t remember what it was like… more like we didn’t want to remember it, but we all had individual “moments” we remembered. One nurse said that she couldn’t remember anything about those weeks, but vividly described an incident in which two young patients coded in the same room and they had to choose which one to intubate first and which one to let die.
A social worker recalls helping a group of nurses communicate with a patient who spoke Greek and was isolated and scared, they didn’t have to care so much, she said, but it was the act of caring so hard that maintained their sanity.
I recall the surreal nature of one of our make-shift ICUs towards the end of the first wave, messy, music from phones in the background, “bunny suits” tied around everyone’s waist (they are hot to wear all day).
When these snippets of shared memories are recalled, everyone looks the same, they get glassy eyed, as if peering into a dark distant place, then everyone says the same things.
“I can’t remember much about it.”
“It’s too soon-I don’t want to think about it.”
“I had no one to talk about this with anyway. “
“It pisses me off that everyone outside is bitching and moaning about being BORED!”
“I’m scared, I don’t think I could do it again. But I’m scared that we’re gonna have to, no one is paying attention!”
I don’t know how I’ll be able to do it again, but I will… as will everyone else, no matter how scared they are. It’s what we do.
Covid Update
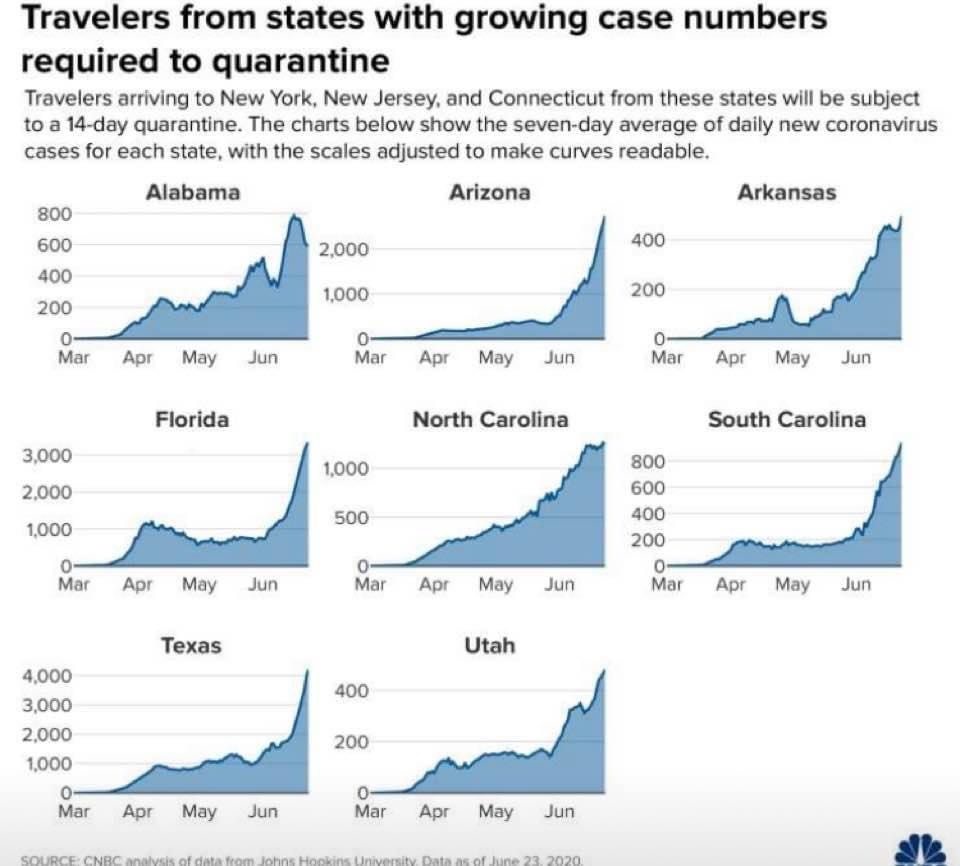
So, I don’t care what you think of New York or it’s governor, New York and the Northeast (except Vermont) has done an amazing job in decreasing cases of Covid.
I fear for all those states that thought we were joking or that we were over dramatic “snowflakes” ( I invite you to see the refrigerated trucks behind the hospital). You are now being hit with it worse than we were.
Wear all the PPE.
I address the new Covid Warriors (healthcare workers) :
Patients should get high flow O2 and lay them prone. All of the meds we have now DON’T WORK!
Isolation is important as is hand hygiene.
Eat well, sleep, wear your mask it’s not political, it’s reality, exercise. Keep relative isolation from vulnerable family members.
Scrubs, head covers with buttons on the sides for the mask straps (look on Etsy) and “Covid sneakers” that you change out of outside your house and throw in the wash before walking in.
Be good to yourself, it’s gonna suck and you’ll likely end up as damaged as we are in the NE. We’ll be here when you need help like you helped us.
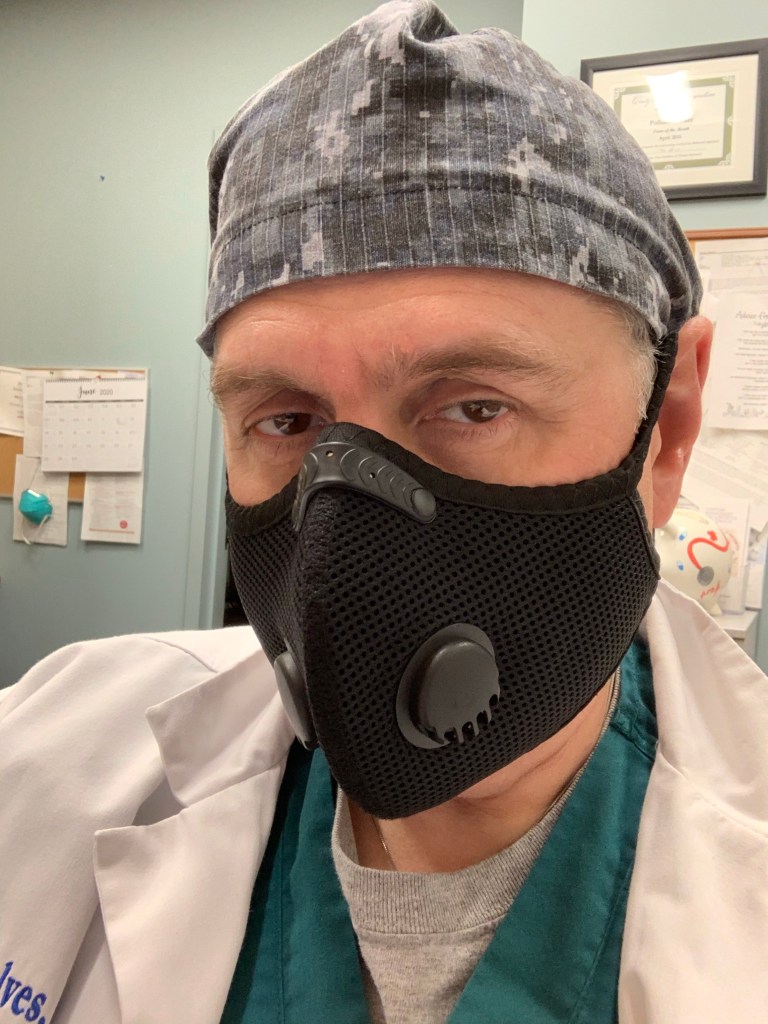
New Mask
On a not serious note, I got a new mask.
Base Camp Mask
Since we’re all going to need masks for the foreseeable future, I ordered a very cool looking and comfortable mask. It is super comfortable with a Velcro strap around the back of the neck (takes the strain off the ears) very breathable with replaceable filters inside.
Called Base Camp masks, it’s good quality, solid shipping and less than 40 dollars.
You’ll spend more on boxes of cheap masks of poor quality that don’t look near as cool. Btw, I’m not getting paid to show you the mask, I just think it’s cool.
As always, wash ya hands, wear a mask, social distance, and love each other… we are all we have.
In the months of March and April, I noticed a curious thing. Whenever I would be outside at night (usually to take out the trash), I would stop and stand very still and listen.
It was dead silent.
There is always a background hum to what we call civilization. Back in High School, our Social Studies teacher took us to the roof of the school and had us listen to it. When I was young I used to love to go up to the roof of the apartment building and listen to it… the hum of the cars, airplanes, ambulances, whatever, it was always there.
Even after 9 11, when all the air traffic was down, the hum was still there.
But during these last two months it was gone. Replaced by an introspective quiet, the absence of useless motion, almost a protective blanket of quiet lest the virus come and get you.
Over the last few days, starting with the slow reopening of Long Island, the growing realization that there is Spring in the air, and the tragic murder of George Floyd with the ensuing protests and completely unaffiliated opportunistic looters, the quiet is gone.
I stood outside and the hum was back.
Gone was the introspection.
Gone was the protective blanket of silence, replaced with white hot anger and the realization that no matter what Nature throws at us, the worst enemy humanity has is itself.
The diseases of Racism, Hatred, Opportunism, and Cruelty have pushed Covid almost to the background.
The mask a mere part of the uniform we all wear to be out in the world.
Covid is still here
I fear that we will see another mini surge in cases with all the protests. I hope not.
There are stillno effective treatments.
We are sending ventilators to Russia (as well as useless Hydroxychloroquine).
And there is the injection of the “culture war” into the basic public health measure of wearing masks.
This Blog is Evolving
I will continue to bring the latest in news of Covid to this blog, but I will also be bringing news of general health, disease specific self care, health and public policy, and a larger perspective to the idea of health writ large.
As Always…
Wash your hands, do not touch your face, social distance, wear the masks! Eat Right, Exercise, and most of all… practice loving each other.
Toleration is NOT the goal, valuing and celebration of each other is the goal.
So the “inside” is looking a lot less like the “inside” every day.
When I resumed these posts, It was at the run-up to the surge in New York (Long Island more specifically) and I watched an orthopedic floor turned into an ICU, I saw nice clean step-down beds (were people go to have some cardiac monitoring – but nothing too “serious”) turned into ICU beds, a holding room for elective surgeries turned into “the fishbowl” of Covid patients were patients watched each other suffocate, and even ambulatory surgery units turned into Covid – care floors.
Like the receeding tide, I am seeing units being returned to their former functions, being made “clean” again. More and more, we are allowing families to at least come and see their sickest relatives before they are necessarily near death. We are even going to open a new cafeteria expansion next week (3 months late because of Covid).
There is a sort of strange melancholy to this process, as the huge bags of “dirty” supplies get thrown out and the rooms are “terminally cleaned” it feels like the day after christmas, after the superbowl, after the world series… the world returning to whatever passed for normal, the exploits and adventures spoken only in “remember whens”.
I look at the sparkling clean rooms and still see the hundreds of patients who suffered and died in them and I don’t want them to be forgotten, their suffering should not have been in vain.
And then I see the crowds rushing to bars and swimming pools and such flouting common-sense self protections and think, “yeah they did die in vain, and it is going to happen again, somewhere else if not here”.
I want it to be over.
I am afraid it is not.
As Always
Wash your hands
Don’t touch your face
Wear a mask… you aren’t freaking superman / captain marvel.
Exercise, eat right.
Love one another, hate doesn’t make anyone better.
It is rare and NOT widespread, this post is for informational purposes only.
In the last week there has been the identification of a pediatric syndrome that seems to be associated with Covid 19 infections in children.
It appears to be an inflammatory reaction by the body to the Covid virus. As we’ve discussed in previous posts, in adults a good bit of the damage appears to come from the body’s immune system attempting to eradicate the virus without the proper tools (antibodies) and just lobbing non-specific inflammatory “bombs” everywhere.
Unfortunately, this looks to be a similar thing but accelerated. It is still early and the condition is still not fully understood, but I’m putting out the information on Pediatric Multi-system Inflammatory Syndrome from NYC Health and Hospital Corp. for your consideration.
As always, please wash hands, don’t touch face, social distance and wear masks in public. Please follow the advice of the local heath departments and the CDC.
They really care about your health and the health of your children
Fact Sheet: Pediatric Multisystem Inflammatory Syndrome What is pediatric multisystem inflammatory syndrome? Pediatric multi-system inflammatory syndrome (PMIS) is a new health condition appearing in children in New York City (NYC) and elsewhere. Some doctors think the condition is related to having coronavirus disease 2019 (COVID-19), but the connection is still not clear. PMIS is like other serious inflammatory conditions such as Kawasaki disease and toxic shock syndrome. Children with PMIS can have problems with their heart and other organs and need to stay in a hospital to receive support in an intensive care unit. PMIS is a rare condition. However, because it is life-threatening, it is important that parents know the signs and symptoms, so they can get help right away. What are the signs or symptoms of PMIS? Most children have fever (temperature of 100.4 degrees F or 38.0 degrees C or greater) lasting several days, along with other symptoms. Common symptoms include: • Irritability or sluggishness • • Abdominal pain without another explanation • Diarrhea • • Vomiting • Rash • • Conjunctivitis, or red or pink eyes When should I call my child’s doctor or get emergency care? You should call your doctor immediately if your child becomes ill and about any signs or symptoms your child has and use that information to recommend next steps. If your child is severely ill, you should go to the nearest emergency room or call 911 immediately. Is PMIS contagious? PMIS is not contagious, but it is possible that your child has COVID-19 or another infection that may be contagious. This is why hospitals will take infection control measures when treating your child. Is there a treatment for PMIS? Currently, children with PMIS are being treated with different therapies, including intravenous immunoglobulin and steroids. These drugs help reduce the body’s immune response that causes the inflammatory syndrome. Children are also being given other medications to protect their heart, kidneys and other organs. How can I prevent my child from getting PMIS? Although we do not know yet if PMIS is related to COVID-19, you should still take steps to prevent your child from being exposed to COVID-19. Face coverings, hand hygiene, and physical distancing are the best way to prevent COVID-19. Children with underlying medical conditions can be at higher risk for poor outcomes of COVID-19, so you should make sure they follow COVID-19 prevention measures. The NYC Health Department may change recommendations as the situation evolves.
“Perseverence is the hard work you do after you get tired of doing the hard work you already did…“**
Covid – 19 in May 2020
There’s an old expression that people use when describing the attempt to bring change to an organization or group while not disrupting the function of the group, “it’s like building a plane while its in the air”.
Yeah, it’s on fire.
In the case of the medical response (we’ll not even get into the national political response) to the COVID – 19 pandemic, we’re trying to build the airplane while its in the air… and its on fire too.
Unfortunately, the medical response has initially been mixed in with the politics and considering that we had nothing to treat this disease at the begining, didn’t harm the response as much as merely confuse the hell out of the general public.
Let’s get to it
To work
What I will do in this post is to review the latest on the drug therapies that we have available and I will separate what is fact-based vs what is my opinion based on what I know and extrapolations.
Hydroxychloroquine
The initial hoopla about this drug comes from early Chinese reports. There were also some communications from France and Italy in which they claimed that there was some decrease in the viral load in the sputum (mucus, spit, phlegm) of people who were given this drug. Why did you give a drug that has no anti-viral properties to these patients? Did the lower viral load improve symptoms? Did the lower viral load improve survival?
The answers (after someone collated and finally looked at the reults) were that 1) they didn’t exactly know why they did it, 2) they were very few of them anyway, 3) the decreased viral load wasn’t significantly (statistically) decreased, and 4) it didn’t seem to improve symptoms nor survival.
So bottom line, it doesn’t work (it never did), it has horrible side effects (including death), and it is a complete waste of time.
Azithromicin
Essentially the innocent bystander in this whole thing, it was used as an adjunct (can something that doesn’t work be used to help another thing that doesn’t work?) to Hydroxychloroquine in the early trial and error phase of Covid treatment. It has an unfortunate side effect of altering the EKG which is usually not a problem as it is given for five days only and usually in relatively healthy people, but in sick patients taking Hydroxychloroquine it was a potentially lethal combination.
Bottom line, it’s good for sinusitis and mild bacterial infection but not COVID.
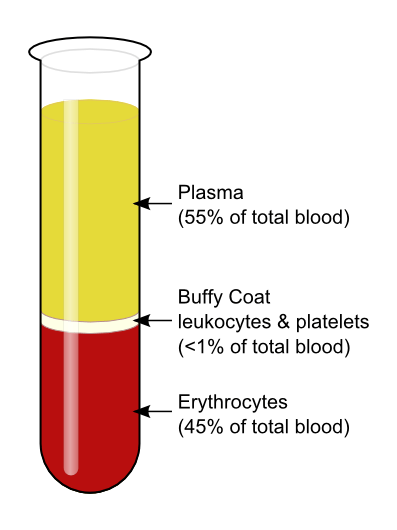
Convalescent Plasma
This is an old stand-by of treating a viral type disease that dates back to 1883 when the different components of blood were discovered. The theory goes back even further to the idea of animism, in that the blood of a survivor must have in it the makings of a survivor.
In a more up-to-date sense, we know this to be true as the person who survives a serious infectious disease does indeed make antibodies to that infectious agent. What we don’t know is if these antibodies will shorten the disease, improve symptoms, or improve survival.
It is being given to severely ill patient’s in hospitals. It is intravenous. Plasma is also very tightly controlled and only given by strict criteria. The reason for this is that the blood plasma has many other components such as coagulation factors and such that could in and of themselves be dangerous. It may also be possible to cause allergic reactions in the recipient.
Bottom Line: It is being given. We don’t know when is best, we don’t know the optimal dosage, and we don’t know if it is doing any good. (Opinion: I wish I could say that I saw great improvement in these severely ill patients, but I haven’t). We remain hopeful that this will be an important part of treatment for now. More data to come.
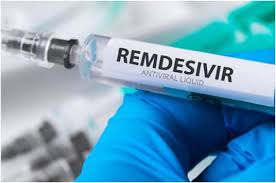
Remdisivir
Self explanatory
Originally developed as a broad spectrum (general purpose) anti-viral for Ebola, this drug interferes in the reproduction of the viral mRNA (the chemical that produces more virus) by messing with the mechanisms that hijack the reproducive mechanisms of the host cells. It is not a cure, but it does slow down the replication of the virus, which in turn preserves more of the body’s own native cells, presumably giving the body time to make antibodies.
Bottom Line: It is still strictly controlled. It is intravenous. Since we aren’t really sure when to give it, and how much, we are still sticking to the study criteria that the manufacturers have laid out. In my opinion, this drug would be most useful when given very early in the illness when the virus is first making it’s attack on the body through the lungs. As it is, we don’t have enough drug (as of this writing, there are close to 1.5 million known cases of COVID – 19 in the US alone and if given more than once -protocols are now for twice daily for 5 days – that would be 15 million doses that would be needed tomorrow) to begin to give it to everyone who will eventually need it.
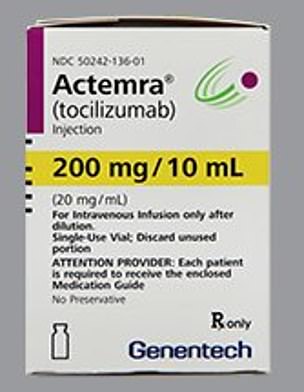
Actemra (Tocilizumab)
Fun Fact: if it ends in a -ab it’s IV, in a -ib it’s a pill
Actemra is a member of the class of drugs called a “biologic”. This is used mainly for people with severe arthritis and it comes with it’s own set of side effects which come from its main function as an immune modulator. What this thing does is to block one of the inflammatory chemicals (The “hand grenades” from an earlier post, called IL-6).
Since the really destructive part of the body’s destructive reaction to COVID – 19 is it’s uncontrolled inflammatory response, a drug that can “diffuse the hand grenades” and blunt the out-of-control inflammatory response would help enormously.
The problem is that there are no studies out yet that use this drug in any numbers that would give us good information on how best to give it and for how long.
Bottom Line: We are giving it in the hospitals. It is IV. It is severely in short supply. I have seen some very good anecdotal (personal experience) responses to this.
Synthesis (Opinion)
From here on in I am giving my opinion on treatment. I believe that we must use a multi-pronged approach to this COVID – 19 constellation of symptoms based on how this disease manifests in humans.
When the virus begins attacking the lungs, a Remdisivir type drug should be started to limit the attacking invader. An Actemra type drug should then be used to dampen the massive inflammatory response of the body that causes the actual damage to the tussues (especially distant damage) and then plasma might be useful as an adjucnt to the initial therapy.
Only by using all the tools available to us will be able to temporize and buy time and save lives until a vaccine is created that will help us land the plane (that was on fire) safely.
In future posts I will discuss any changes to the above indications or medications as they come in and out of favor but I won’t rehash any of the older information. Unfortunately, this virus looks to be sticking around for awhile and I don’t want you to get bored.
As always
Wash your hands. Don’t touch your face. Exercise. Eat right. Social distance. Wear a mask in public. Be kind and be patient.
The opinions expressed here are mine and do not reflect the opinions of any medical organization.
In the last week or so, the pace of life on the “inside” has been marked by a steady change in how the world works for us.
Early on, it was preparing for the surge, then it became the overwhelming fear and frustration as we were seemingly swallowed by the onslaught. However, over the last week it’s different. We seem to be settling in for the long haul. Its NOT going to be over soon. We’ll push it to certain areas of the hospital, but it is not going away.
In an earlier post, I’d said that we seemed to be getting a handle on it… it was naive of me to say that. We had discovered the rhythm and the pattern of the illnesses but not exactly how to beat it.
The Virus
Paths of Disease
The asymptomatic (no symptoms) form is as if you had nothing, maybe a little sniffle at most. You get better on your own but hell… you didn’t know you had it. You remain infectious.
The mild form is the at home version that you hear about… Chris Cuomo on CNN and such. It looked awful, and it is, but the fevers and shortness of breath are survivable.
There’s the moderate reaction to the virus which is like the mild form but with the extra added attraction of hypoxemia (low blood oxygen) and shortness of breath that often leads people to come to the ER. These folks are usually admitted, given oxygen, vitamins, whatever the cocktail (of medications and vitamins) of the day, made to lay down on their bellies (the prone position) and watched to see if they get better or not.
From there it splits:
1) You get better and are sent home on oxygen to recover.
2) It Gets Worse.
If you get better, you get better. If it gets worse you go one of two ways (generally):
The Long Slow Burn:
You cough and get low blood oxygen. Over time the lung damage causes you to need higher doses of oxygen. The lucky ones eventually heal and are weaned off the oxygen. If you are not lucky, you get stuck at this level. There are many people stuck in the hospital at this level.
The Long Blaze:
Your lungs can’t supply the body with oxygen and you get intubated and put on a ventilator. This can be for a long time. Since this whole deal has only been going on for around two months we don’t know how long, but the longer you are on a ventilator, the worse it is. There are many people who come off so there is hope, its getting better the more experience we get.
Anticoagulation
So there is talk online about Covid – 19 causing abnormal blood clotting and people taking blood thinners. Whenever someone is seriously ill, there is a chance of blood clots. This bugger has a chemical that causes the clotting system to go haywire in its envelope, so during critical illness there are blood thinners used. DO NOT TAKE BLOOD THINNERS TO PREVENT COVID – 19.
Medications
Hydroxychloroquine (Plaquanil) – NO
Zithromax – Not for Covid
Zinc – 50 mg of elemental Zinc for maximum of 12 weeks max
Vitamin C – Maximum of 2,000 mg a day
We’re Getting there
Multivitamins – Sure why not?
Plasma – plasma from people who have had the disease. We don’t know dosages and we don’t know if it works.
We are giving it in hospital only.
Remdisivir – Developed for Ebola and has been shown to decrease time of active disease. It is only IV and we don’t yet have the actual correct dosages yet.
But this is actually looking good.
Bottom Line
– Wash your hands
– Wear a mask in public
– Practice Social Distancing
-Exercise
-Stop Smoking
-Eat Right
-Stay Away from stuff that can stress you out (I’m looking at you News and Facebook).
I was tested three days ago for the antibodies for Covid-19.
I came up negative.
This is a good thing I tell myself, as I try to process and come to terms with, “That horrible cough and fatigue I had over two months ago” must have been just a bad cold. What it means from a scientific point of view is that I haven’t had an exposure that resulted in my getting an infection that would have prompted my immune system to mount an antibody response within the last two weeks.
So my daily exposure to Covid-19 at the hospital (as limited as it is compared to all the real front line nurses, doctors, and especially nurse’s aides) has not given me an infection.
So yay for PPE!
Yay also for having an office to which I can escape to after rounds, even though it smells like Clorox and has PPE bags hanging from the walls, it is an area to escape from the crushing presence of the virus. I feel for those in the ED and Covid units who have little escape.
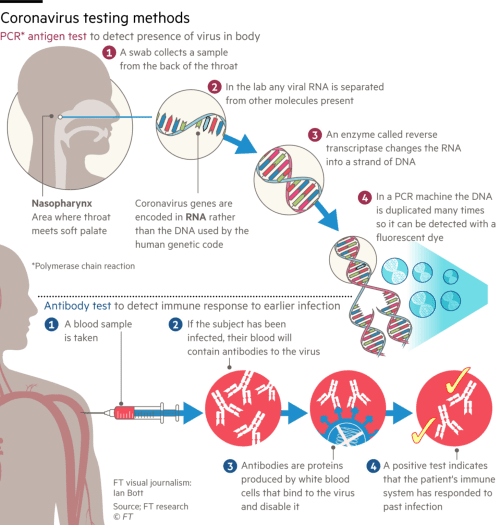
Corona virus testing methods
As expected, one of my colleagues in the office has also tested negative and I expect the other two to test negative as well.
This does NOT mean that we can’t get it though, so the idea of have a “card or an app” that identifies a person who is negative as “safe” is silly.
It just means that I haven’t gotten an infection in the last 2 weeks. It doesn’t mean that I don’t currently have a sub-clinical (no symptoms) infection and I might be positive in two weeks, or even that I am not currently infectious. So there’s that.
And there’s the quandary.
Obviously, those of us who are negative are now in the “try not to get it” game. I can assure you that you don’t want to take the chance on getting it and being that lucky small percent that get asymptomatic infection.
If, on the other hand, you are positive and have antibodies, you have the option of getting a good quantitative (to see the levels of antibodies) test, and donating plasma to see if it helps, or not.
However, does having antibodies give you any immunity? Can you get it again? How long would this immunity (if it is a thing) last? Would it be partial (like making a bad infection less difficult) or total?
We don’t know.
Some viruses give a strong immunity and some don’t. I personally have had Rubella (German Measles), four times in my life until I started getting MMR vaccine (yeah there was a time that was not a thing – I’m old ok?) because the Rubella disease didn’t give me long lasting immunity.
Granted, if this virus gave no immunity (of any sort) it would be one of very few that didn’t, but the issue is, we just don’t know.
Testing everyone…
Testing Everyone
So, since we didn’t get ahead of this thing at the start (for whatever reason… lets not get into it), we have to play the cards we’re dealt .
The only way to know who is “safe” and who is “contagious” and more importantly, what is the prevalence of the virus is to test everyone repeatedly.
Without this, we won’t know what the true infection rate is, we won’t know what the true death rate is, we won’t know how the disease spreads, and we’ll stumble around just watching some people live and some people die like we did in the 1960’s (I was there, it sucked – routine male sterility with mumps, routine death and blindness from measles, paralysis from polio, etc). So yeah we test everyone, maybe on an every 6 month basis, but this should not in any way be used to restrict anyone from their rights, just as a tool to understand the disease and control its spread.
The early numbers we have (which stink because we haven’t tested enough) don’t show that 50% of the population that gets Covid gets antibodies but like I said, these numbers can change when we actually start testing people en masse.
Until a vaccine is done, everyone wears a mask and presumes the other person is infectious.
Kind of a rough way to live, not to mention a rough way to thrive, but unless you are willing to absorb three to five million deaths in the US alone (like they would have been ok with in the 50’s and 60’s because we didn’t have anything else) it is what we are going to have to do.
By the way, if your answer is that you’d be ok with it, you’ll be doing it at home by yourself, because we have seen that the medical system, such as it is, can barely keep up with the current level of dying patients.
Next Time: Anticoagulation For Asymptomatic Cases?
Ok so we know how Covid -19 works and that it attacks the lungs (and kidneys). Why do some people end up on Ventilators and why do some end up not needing them?
Short answer: We don’t know.
That is what makes this thing so difficult to predict and scary. It isn’t “I’m young and healthy, I’ll be ok!” it seems to be either some kind of genetic thing or viral load or something that causes some people – regardless of age or health to have respiratory failure and some people to be OK. I’ve seen personally 96 year olds with all kinds of co-Morbidities (other things going on other than Covid), get better and go home and a 37-year-old otherwise healthy man die of respiratory failure. So yeah, we don’t know.
But before we talk about what ventilators are and why we use them, we need to get on the same page.
Definitions
Respirator: A form of PPE (personal protective equipment) that has filters and generally (but not always) a motor and a source of additional air – like a scuba tank . Think of the air tanks and masks worn by firefighters, those are respirators. There are smaller versions that are worn by surgeons in hospitals when in a toxic situation – usually in the movies.
Ventilator: A machine that blows air (of differing oxygen percentages and pressures) into the lungs and takes the air out. We call these things ventilators because what they do is push air in and take air out (Ventilate the lungs) – they DON’T inject air or oxygen into the lungs.
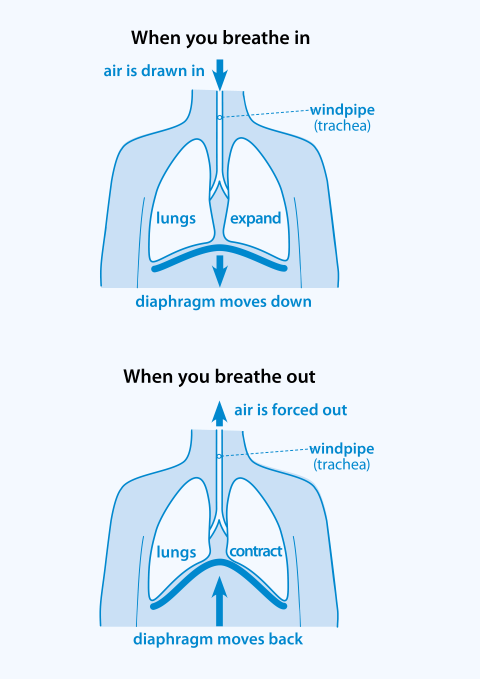
How we breathe naturally
Natural Breathing
When we breathe naturally our diaphragms (the wide muscle between your chest and your abdomen) contract (move down) and since the only way into your lungs is through your throat (trachea), the air whooshes in. When we breathe out, the diaphragms relax and the air comes out.
That’s the natural way.
When we use ventilators, we DON’T do it the natural way. Instead of letting the diaphragms and the body take in air like the tides (in and out), we stick a long plastic tube into the throat, between the vocal cords, inflate a little balloon at the end of the tube to seal it up and blow a certain amount of air with a certain amount of oxygen in to it and then take it out.
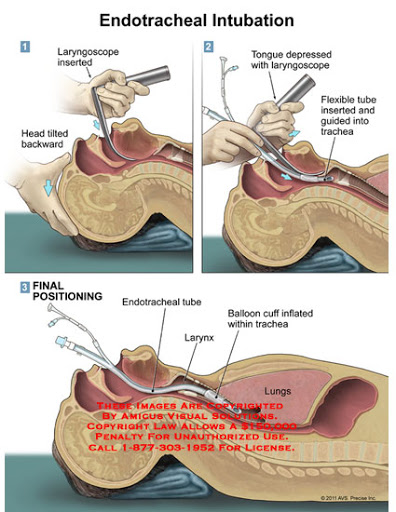
Intubation
When someone is intubated (like during surgery or for a serious illness like Covid), it happens like in the diagram below.
A doctor puts a thing called a laryngoscope which is basically a large long spoon, that is used to move the tongue out of the way and while staring intently (and getting all kinds of droplets all over their face) slides the tube into the trachea.
The balloon is inflated to prevent movement and to seal it off from outside stuff and then it is taped in place on the face. You cannot talk or eat when you are intubated.
In the OR ( Operating Room) this is done in very controlled circumstances, quiet with music in the background – everyone smiling.
In Covid, there is usually anxiety, fear, and a good bit of yelling. These Docs and Respiratory Therapists are pro’s though and they get it done successfully. Once you are intubated, you are put on a mechanical ventilator.
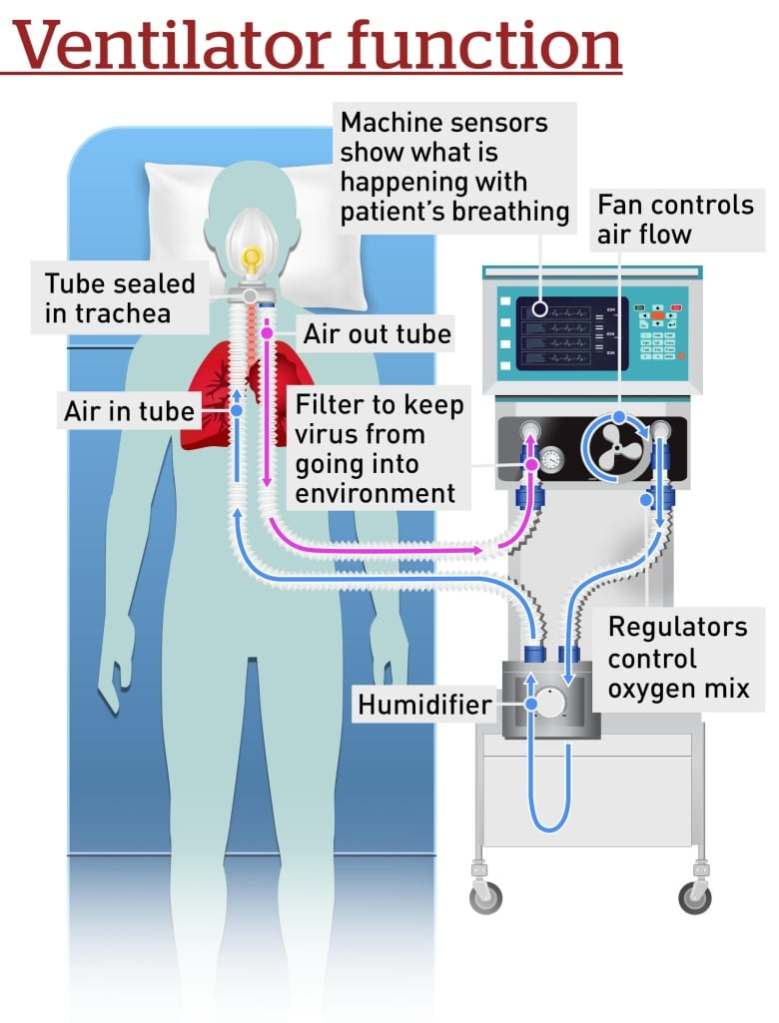
Ventilators
Basics of a Ventilator
Ventilators consist of several parts. There is the tube that comes out of the patient that is split (soon after it comes out of the person) into the tube that brings the air into the person and the tube that takes air away.
They have built in filters to keep bad stuff (including viruses) from spewing into the air.
There is a fan that is connected to a bunch of electronics that attaches to oxygen tanks. The electronics monitor how much is going in, the temperature of the air, and a whole bunch of other complicated stuff. The fan pushes air through a humidifier (dry air is bad) and then into the patient (like a pump pushes air into your tires at the gas station).
So air (mixed with oxygen and humidification) goes in, and then it lets the air out. Room air has 21% Oxygen (the rest is carbon dioxide, nitrogen, and other gasses). If the body doesn’t have enough oxygen in the blood (there are ways to measure that), then the Docs turn up the oxygen in the air that goes into the lungs, they can go all the way to 100%. When you get better, then the Docs take the tube out.
Fancy ICU ventilator on the left, ummm… less fancy government ones on the right.
So Why?
In the last post we talked about how Covid attacks the lungs (and kidneys). When the air sacs get damaged, the body can’t take in enough oxygen from the 21% floating around in the air. It also can’t get rid of the Carbon Dioxide (CO2) that our bodies produce (we make a lot of that). So, in order to do both, the person starts to breath real hard. They also need to move the blood around faster so the heart begins to beat faster.
The problem is that in Covid, the person is coughing a lot.
If they can’t breath enough through the coughing to keep their oxygen in their blood at normal levels (between 88% and 100%), Docs will start them on Oxygen, usually through a face mask.
If the oxygen in their blood is still too low, the person begins to tire out and they will need help to breath. So before this happens they get intubated and put on ventilators.
This isn’t a great sign.
But, there is hope. As we learn more about this bastard, we figure out what works and what doesn’t. We are gentler and have learned that we can tolerate lower oxygen levels.
I’ve seen many people come off ventilators (we call them “vents” – so you’ll sound cool to your friends), and the more good real treatments we get, the more people will be coming off.
Bottom Line
Wash your hands like a maniac… please.
Wear a face mask when you go out anywhere that you might run into people where you have to get closer than six feet.
Don’t touch your face.
When the shortages go away, get hand sanitizer and use it all the time.