In the last week or so, the pace of life on the “inside” has been marked by a steady change in how the world works for us.
Early on, it was preparing for the surge, then it became the overwhelming fear and frustration as we were seemingly swallowed by the onslaught. However, over the last week it’s different. We seem to be settling in for the long haul. Its NOT going to be over soon. We’ll push it to certain areas of the hospital, but it is not going away.
In an earlier post, I’d said that we seemed to be getting a handle on it… it was naive of me to say that. We had discovered the rhythm and the pattern of the illnesses but not exactly how to beat it.
The Virus
Paths of Disease
The asymptomatic (no symptoms) form is as if you had nothing, maybe a little sniffle at most. You get better on your own but hell… you didn’t know you had it. You remain infectious.
The mild form is the at home version that you hear about… Chris Cuomo on CNN and such. It looked awful, and it is, but the fevers and shortness of breath are survivable.
There’s the moderate reaction to the virus which is like the mild form but with the extra added attraction of hypoxemia (low blood oxygen) and shortness of breath that often leads people to come to the ER. These folks are usually admitted, given oxygen, vitamins, whatever the cocktail (of medications and vitamins) of the day, made to lay down on their bellies (the prone position) and watched to see if they get better or not.
From there it splits:
1) You get better and are sent home on oxygen to recover.
2) It Gets Worse.
If you get better, you get better. If it gets worse you go one of two ways (generally):
The Long Slow Burn:
You cough and get low blood oxygen. Over time the lung damage causes you to need higher doses of oxygen. The lucky ones eventually heal and are weaned off the oxygen. If you are not lucky, you get stuck at this level. There are many people stuck in the hospital at this level.
The Long Blaze:
Your lungs can’t supply the body with oxygen and you get intubated and put on a ventilator. This can be for a long time. Since this whole deal has only been going on for around two months we don’t know how long, but the longer you are on a ventilator, the worse it is. There are many people who come off so there is hope, its getting better the more experience we get.
Anticoagulation
So there is talk online about Covid – 19 causing abnormal blood clotting and people taking blood thinners. Whenever someone is seriously ill, there is a chance of blood clots. This bugger has a chemical that causes the clotting system to go haywire in its envelope, so during critical illness there are blood thinners used. DO NOT TAKE BLOOD THINNERS TO PREVENT COVID – 19.
Medications
Hydroxychloroquine (Plaquanil) – NO
Zithromax – Not for Covid
Zinc – 50 mg of elemental Zinc for maximum of 12 weeks max
Vitamin C – Maximum of 2,000 mg a day
We’re Getting there
Multivitamins – Sure why not?
Plasma – plasma from people who have had the disease. We don’t know dosages and we don’t know if it works.
We are giving it in hospital only.
Remdisivir – Developed for Ebola and has been shown to decrease time of active disease. It is only IV and we don’t yet have the actual correct dosages yet.
But this is actually looking good.
Bottom Line
– Wash your hands
– Wear a mask in public
– Practice Social Distancing
-Exercise
-Stop Smoking
-Eat Right
-Stay Away from stuff that can stress you out (I’m looking at you News and Facebook).
I was tested three days ago for the antibodies for Covid-19.
I came up negative.
This is a good thing I tell myself, as I try to process and come to terms with, “That horrible cough and fatigue I had over two months ago” must have been just a bad cold. What it means from a scientific point of view is that I haven’t had an exposure that resulted in my getting an infection that would have prompted my immune system to mount an antibody response within the last two weeks.
So my daily exposure to Covid-19 at the hospital (as limited as it is compared to all the real front line nurses, doctors, and especially nurse’s aides) has not given me an infection.
So yay for PPE!
Yay also for having an office to which I can escape to after rounds, even though it smells like Clorox and has PPE bags hanging from the walls, it is an area to escape from the crushing presence of the virus. I feel for those in the ED and Covid units who have little escape.
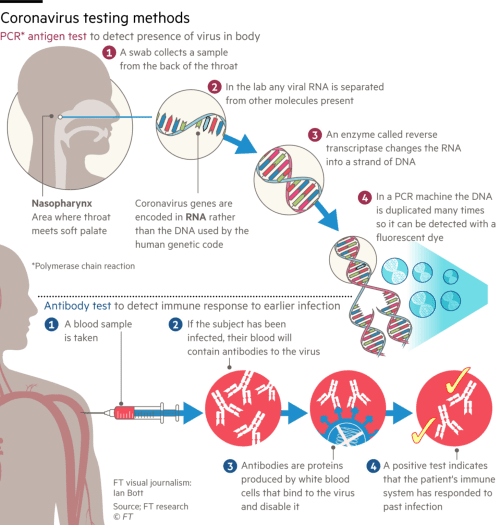
Corona virus testing methods
As expected, one of my colleagues in the office has also tested negative and I expect the other two to test negative as well.
This does NOT mean that we can’t get it though, so the idea of have a “card or an app” that identifies a person who is negative as “safe” is silly.
It just means that I haven’t gotten an infection in the last 2 weeks. It doesn’t mean that I don’t currently have a sub-clinical (no symptoms) infection and I might be positive in two weeks, or even that I am not currently infectious. So there’s that.
And there’s the quandary.
Obviously, those of us who are negative are now in the “try not to get it” game. I can assure you that you don’t want to take the chance on getting it and being that lucky small percent that get asymptomatic infection.
If, on the other hand, you are positive and have antibodies, you have the option of getting a good quantitative (to see the levels of antibodies) test, and donating plasma to see if it helps, or not.
However, does having antibodies give you any immunity? Can you get it again? How long would this immunity (if it is a thing) last? Would it be partial (like making a bad infection less difficult) or total?
We don’t know.
Some viruses give a strong immunity and some don’t. I personally have had Rubella (German Measles), four times in my life until I started getting MMR vaccine (yeah there was a time that was not a thing – I’m old ok?) because the Rubella disease didn’t give me long lasting immunity.
Granted, if this virus gave no immunity (of any sort) it would be one of very few that didn’t, but the issue is, we just don’t know.
Testing everyone…
Testing Everyone
So, since we didn’t get ahead of this thing at the start (for whatever reason… lets not get into it), we have to play the cards we’re dealt .
The only way to know who is “safe” and who is “contagious” and more importantly, what is the prevalence of the virus is to test everyone repeatedly.
Without this, we won’t know what the true infection rate is, we won’t know what the true death rate is, we won’t know how the disease spreads, and we’ll stumble around just watching some people live and some people die like we did in the 1960’s (I was there, it sucked – routine male sterility with mumps, routine death and blindness from measles, paralysis from polio, etc). So yeah we test everyone, maybe on an every 6 month basis, but this should not in any way be used to restrict anyone from their rights, just as a tool to understand the disease and control its spread.
The early numbers we have (which stink because we haven’t tested enough) don’t show that 50% of the population that gets Covid gets antibodies but like I said, these numbers can change when we actually start testing people en masse.
Until a vaccine is done, everyone wears a mask and presumes the other person is infectious.
Kind of a rough way to live, not to mention a rough way to thrive, but unless you are willing to absorb three to five million deaths in the US alone (like they would have been ok with in the 50’s and 60’s because we didn’t have anything else) it is what we are going to have to do.
By the way, if your answer is that you’d be ok with it, you’ll be doing it at home by yourself, because we have seen that the medical system, such as it is, can barely keep up with the current level of dying patients.
Next Time: Anticoagulation For Asymptomatic Cases?
Ok so we know how Covid -19 works and that it attacks the lungs (and kidneys). Why do some people end up on Ventilators and why do some end up not needing them?
Short answer: We don’t know.
That is what makes this thing so difficult to predict and scary. It isn’t “I’m young and healthy, I’ll be ok!” it seems to be either some kind of genetic thing or viral load or something that causes some people – regardless of age or health to have respiratory failure and some people to be OK. I’ve seen personally 96 year olds with all kinds of co-Morbidities (other things going on other than Covid), get better and go home and a 37-year-old otherwise healthy man die of respiratory failure. So yeah, we don’t know.
But before we talk about what ventilators are and why we use them, we need to get on the same page.
Definitions
Respirator: A form of PPE (personal protective equipment) that has filters and generally (but not always) a motor and a source of additional air – like a scuba tank . Think of the air tanks and masks worn by firefighters, those are respirators. There are smaller versions that are worn by surgeons in hospitals when in a toxic situation – usually in the movies.
Ventilator: A machine that blows air (of differing oxygen percentages and pressures) into the lungs and takes the air out. We call these things ventilators because what they do is push air in and take air out (Ventilate the lungs) – they DON’T inject air or oxygen into the lungs.
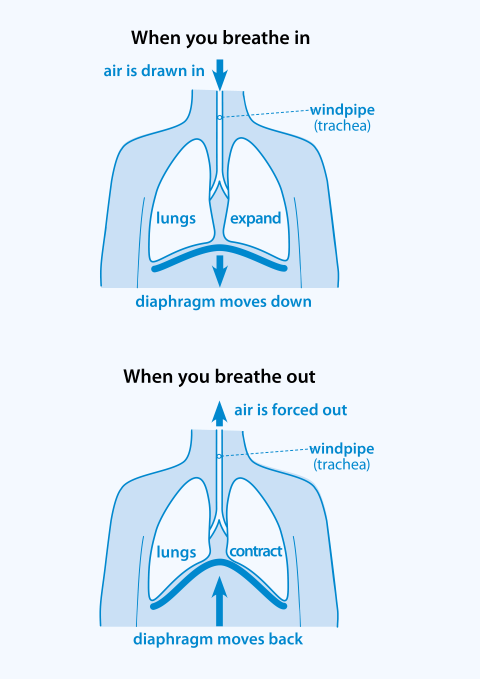
How we breathe naturally
Natural Breathing
When we breathe naturally our diaphragms (the wide muscle between your chest and your abdomen) contract (move down) and since the only way into your lungs is through your throat (trachea), the air whooshes in. When we breathe out, the diaphragms relax and the air comes out.
That’s the natural way.
When we use ventilators, we DON’T do it the natural way. Instead of letting the diaphragms and the body take in air like the tides (in and out), we stick a long plastic tube into the throat, between the vocal cords, inflate a little balloon at the end of the tube to seal it up and blow a certain amount of air with a certain amount of oxygen in to it and then take it out.
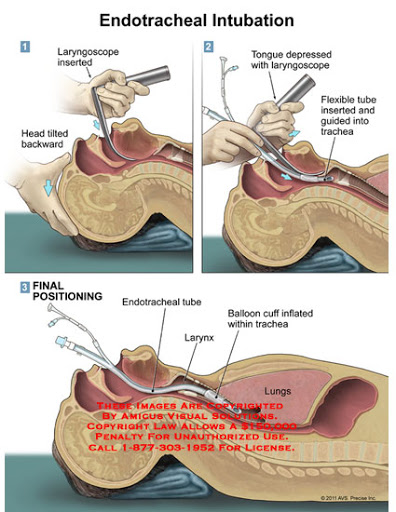
Intubation
When someone is intubated (like during surgery or for a serious illness like Covid), it happens like in the diagram below.
A doctor puts a thing called a laryngoscope which is basically a large long spoon, that is used to move the tongue out of the way and while staring intently (and getting all kinds of droplets all over their face) slides the tube into the trachea.
The balloon is inflated to prevent movement and to seal it off from outside stuff and then it is taped in place on the face. You cannot talk or eat when you are intubated.
In the OR ( Operating Room) this is done in very controlled circumstances, quiet with music in the background – everyone smiling.
In Covid, there is usually anxiety, fear, and a good bit of yelling. These Docs and Respiratory Therapists are pro’s though and they get it done successfully. Once you are intubated, you are put on a mechanical ventilator.
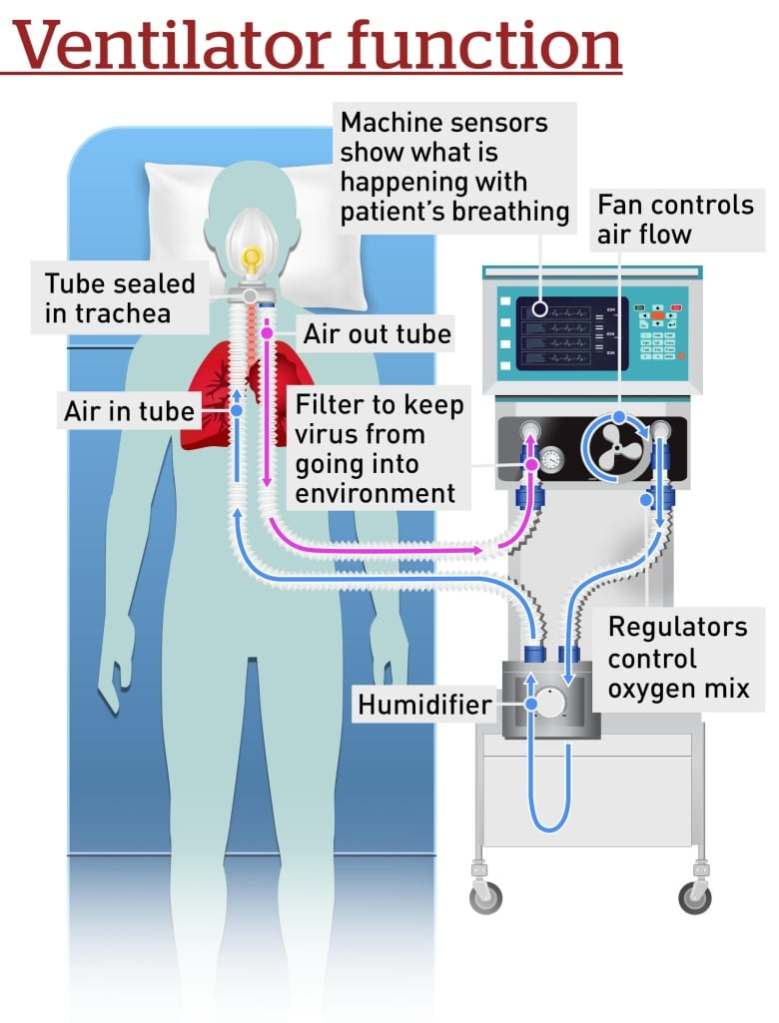
Ventilators
Basics of a Ventilator
Ventilators consist of several parts. There is the tube that comes out of the patient that is split (soon after it comes out of the person) into the tube that brings the air into the person and the tube that takes air away.
They have built in filters to keep bad stuff (including viruses) from spewing into the air.
There is a fan that is connected to a bunch of electronics that attaches to oxygen tanks. The electronics monitor how much is going in, the temperature of the air, and a whole bunch of other complicated stuff. The fan pushes air through a humidifier (dry air is bad) and then into the patient (like a pump pushes air into your tires at the gas station).
So air (mixed with oxygen and humidification) goes in, and then it lets the air out. Room air has 21% Oxygen (the rest is carbon dioxide, nitrogen, and other gasses). If the body doesn’t have enough oxygen in the blood (there are ways to measure that), then the Docs turn up the oxygen in the air that goes into the lungs, they can go all the way to 100%. When you get better, then the Docs take the tube out.
Fancy ICU ventilator on the left, ummm… less fancy government ones on the right.
So Why?
In the last post we talked about how Covid attacks the lungs (and kidneys). When the air sacs get damaged, the body can’t take in enough oxygen from the 21% floating around in the air. It also can’t get rid of the Carbon Dioxide (CO2) that our bodies produce (we make a lot of that). So, in order to do both, the person starts to breath real hard. They also need to move the blood around faster so the heart begins to beat faster.
The problem is that in Covid, the person is coughing a lot.
If they can’t breath enough through the coughing to keep their oxygen in their blood at normal levels (between 88% and 100%), Docs will start them on Oxygen, usually through a face mask.
If the oxygen in their blood is still too low, the person begins to tire out and they will need help to breath. So before this happens they get intubated and put on ventilators.
This isn’t a great sign.
But, there is hope. As we learn more about this bastard, we figure out what works and what doesn’t. We are gentler and have learned that we can tolerate lower oxygen levels.
I’ve seen many people come off ventilators (we call them “vents” – so you’ll sound cool to your friends), and the more good real treatments we get, the more people will be coming off.
Bottom Line
Wash your hands like a maniac… please.
Wear a face mask when you go out anywhere that you might run into people where you have to get closer than six feet.
Don’t touch your face.
When the shortages go away, get hand sanitizer and use it all the time.
It is April 20 th and it seems to be getting better. We have more Personal Protective Equipment (PPE) and here on Long Island the surge is beginning to slow down. We still have a ton of patients but there is a feeling that we at least know a little bit more about what is going on. To that end let me clear up a lot of mis-information that I have seen on the internet.
What is a Bacteria and What is a Virus?
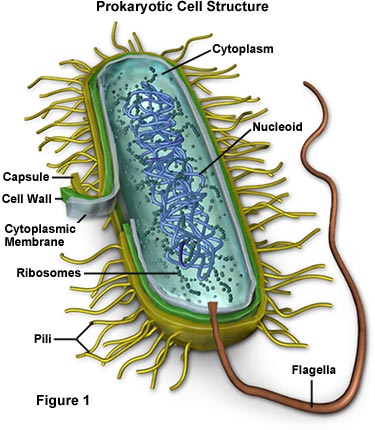
Bacteria
Bacteria are very tiny one – celled plants. When I say that they are plants, I mean that they are individual creatures that have basic characteristics of plants. They eat, they release waste, they reproduce, and they have cell walls (the part that gives vegetables their crunch) and they can alter their environment to make it more comfortable for them.
Bacterial Cell
When we get bacterial infections, it means that these little plants set up housekeeping in a part of your body, such as kidneys, lungs, or throat, then they change the environment by changing the ph (to prevent the body from attacking it) that will allow the group of bacteria to reproduce successfully.
These creatures want to live, and they choose your body as a comfy place to live in. If you live or die does not concern them, but their main purpose is to have a comfortable place to live so they don’t tend to kill you right away.
Viruses
A virus is NOT ALIVE. It is a biological machine whose sole purpose is to reproduce. It consists of a piece of messenger RNA (a tiny strand of chemicals that carries instructions on how to build another virus) with an envelope and a way to inject it into a cell.
Corona Virus the proteins are shaped like a crown (Corona in Latin)
When the virus injects the mRNA into one of your cells, it hijacks the reproductive mechanisms of YOUR cells to reproduce itself. It truly doesn’t care to set up shop, or to make a comfy place because it is not alive. It will break into your cells, take over the reproductive machinery, overload and use up the cell to make more of itself and then burst the cells to spread more of itself.
In the picture above, the spikes such through your cell membranes (animals don’t have cell walls – we don’t crunch) and that yellow string of mRNA shoots through.
In COVID – 19 (COrona Virus that was ID‘ed in 2019), the pink spikes attach themselves to certain areas in the lung cells and the kidney cells.
The Disease
When the virus enters into your respiratory tract (through droplets that people cough out or even spew out when they talk) these things attach to the cells of the airsacs, take them over, burst them, and the viruses spread out into the air and into the blood. The viruses that go out into the air spread to people via droplets or land on surfaces to be picked up by people’s hands and transported onto someone else’s mucus membranes then into their lungs. The virus that goes into the blood, makes its way to the kidneys, attaches there and begins to destroy the kidneys as well as making its way back to the lungs.
Viruses don’t set up shop, they attack and destroy as soon as possible and they can kill quickly.
How The Body Fights It
The body has two ways that it destroys attackers.
The first way is the “soldiers“. The body has cells called White Blood Cells (WBC) which travel the blood stream looking for foreign bodies (bacteria and such) which they engulf and kill using little blobs of acid they carry inside of them.
In order to get the soldiers to the area needed, the body releases certain chemicals (histamines and cytokines – like hand grenades that destroy anything even healthy cells ) that cause leaky blood vessels and causes swelling. These cytokines and WBC also cause fevers that are designed to kill these invaders. Arguably, the purpose of this system is to immediately attack bacteria, surround them and kill them.
The second way are the “snipers“. These cells get intel on these invaders (every single abnormal thing in the body), and through their own mechanisms create magic bullets (antibodies) that target all or part of any invader, effectively preventing the bad guys from attaching at all. This system is set up to attack viruses as well as bacteria. Remember you can put thousands of viruses on the surface of a bacteria… they are that small. So the snipers attack big as well as tiny things. These snipers DEPEND ON INTEL! In other words these cells MUST HAVE SEEN THE INVADER BEFORE. Covid – 19 is a “Novel” Corona Virus, meaning that humans have NEVER SEEN IT BEFORE. So our snipers (the guys responsible for preventing virus attacks) have no magic bullets.
So, Covid – 19 enters your airways, attaches to your air sac cells, does its thing and within hours begins to reproduce and destroy your air sacs and kidney cells.
So the body does what it knows how to do… it sends the soldiers.
It has no Magic Bullets, so what does it do?
It sends LOTS OF SOLDIERS to the lungs and kidneys, along with the chemicals that cause swelling (histamines) and the hand grenades (the cytokines).
Covid – 19 Disease (called “pneumonia” because that is what it looks like on x-ray but not a traditional pneumonia), has 2 phases: 1) the initial phase in which the lung and kidney cells are destroyed and consists of cough, low oxygen, and kidney failure and 2) the “cytokine storm” in which the body doesn’t know what to do and throws “hand grenades” at the virus and in turn helping to destroy more lung and kidney tissue.
Treatments
Treatments that make sense are those that support the body such as oxygen, Remdisivir (a broad spectrum ant-virus created to combat Ebola) that attacks certain parts of viruses (specific anti-viruses like for AIDS don’t work), plasma (that has the “magic bullets” from people who have survived), and Chemicals that fight the cytokines (IL6 inhibitors) are in place and show good promise.
Hydroxychloroquine doesn’t work. Studies have shown that it doesn’t and frankly there is no reason why it should. Zithromax is a nice antibiotic that doesn’t fight a virus. Both of these can cause sudden cardiac death unless prescribed appropriately by a doctor for appropriate reasons. Covid 19 is not it.
Now, aspirin is an anticoagulant that should be used for heart disease. The finding in autopsies that there are micro emboli is to be expected as there is damage to lungs and the clots form as the body tries to heal.
Doctors do use blood thinners during treatment for the prevention of blood clots and there is evidence for using blood thinners to prevent blood clots in the lungs of people who were really sick and survive. But taking high dose aspirin to prevent blood clots may cause you to bleed into your lungs if you are not carefully monitored.
Bottom Line
There is NO CURE.
Only a vaccine will prevent it which is over a year away.
WASH YOUR HANDS or use hand sanitizer.
Cover your face with a mask or scarf when out in public (remember you need to prevent droplets).
Remember no one knows who gets sickest so its not just old people, it can be young people as well.
Use Social distancing (6 ft is the distance droplets go if you cough).
I haven’t written in a few days for three reasons. Firstly I’ve been very tired, the daily work is mentally and physically draining to the point where I sort of just sit and watch life at home flow around me when I’m not at work. Secondly, I’ve had a series of impressive anxiety episodes that I’ve only come to understand now that I’ve come out the other side. I have a Fitbit (I’m not an Apple Watch person yet) and it measures heart rate, exercise, and all that. For the last week, I have had over 45 minutes of “exercise” (heart rate over 100 bpm) and I can assure you I have NOT done any cardio (I wanted to but I fell asleep). I searched the app and found that my heart rate jumped over 100 bpm when I started rounds in the morning and proceeded in fits and starts during the day. That was a bit of an insight that made it easier to realize and control. This results in enough energy to write this post. Thirdly, I have been supremely pissed off.
Idiots
I am not generally critical of fake TV “Doctors” who push diets and therapy and such (everybody needs to make a living) but over the last several days I am astonished at the behavior of two particularly influential peddlers of their own egos.
Dr. Phil (not going to write his whole name because I don’t care) went on TV and in order to gin up his “base”, stated outright that social distancing was not necessary – Jeez what a moron! I read on a popular meme that opening up social distancing because we’ve flattened the curve is like taking off the parachute because we’re slowing down. Dr. Phil, you overinflated egotist, you are a psychologist who used to be a jury profiler and have now peddle stories of nympho 13 year olds… stay in your area of expertise and don’t pretend to be physician.
Dr. Oz (OMG I hate this guy). He went on Fox News and said (he REALLY SAID THIS) that “2% mortality of the total population could die if you open schools, and that is an acceptable outcome to open the economy.” Two percent of the US population is 7 Million people. Think about it… 7 million people!
Both these charlatans went on TV to walk back their BS, likely to try and save what little credibility they have. But, mark my words, they will have shows showing “the horrors of Covid” up close. It’s red meat to these guys.
Finally the President.
OMG
“liberate your state” (?) Seriously?
I fear for my colleagues who will have to dive into the ICU’s in the Mid-West and South when these “patriots” begin filing in and needing intubation. I’m sorry, I’m too old for another round of this (AIDS, SARS, MERS, H1N1, and now Covid), I’m going to sit the next one out thank you very much.
Observations From the Inside
My Associate and I in really big tyvek suits.
Let me disabuse any of my readers from the mistaken idea that life on the inside has gotten any easier.
We have many more discharges than we used to have (the hospital plays “Here comes the sun” when someone gets discharged who had Covid) but there are still many many admissions. Some of whom we can gingerly nurse along keeping them on high flow oxygen and keeping them prone (face-down) and so far what we’ve been doing seems to help them.
Most still fall into catagories of a rapid crash and intubation and mechanical ventilation or long indolent courses that may or may not improve – we don’t really know yet (it’s still developing).
The plateau is like scraping along a bumpy road in a car with no shock absorbers, it’s bumpy, uncomfortable, and potentially dangerous. Every day more and more nursing home patients just die, and our fellow health care workers are taken off the board as they get Covid.
PPE is adequate but NOT what we all learned about in school… and we make all kinds of compromises.
Everyone is tired, and the first line of expert health care workers are being burnt to a crisp. I fear what our souls and hearts will look like when this is all over. I also fear for those who have been “rushed” to graduate into this environment. They will forever know medical care as Covid, and likely suffer intellectual myopia like I did when AIDS swept through the world and Polio was still a major player.
There is too much food being donated to the hospitals (in my opinion) maybe some can go to a food bank or outreach programs to feed those who have lost work.
I truly appreciate the applause and fire trucks, but please… just take care of yourselves and stop calling us heroes and yet make more work for us.
Information
So here is what we know about drugs for Covid so far:
Hydroxychloroquine
Useless and dangerous. Just don’t.
Azithromicin
Might help to address any co-infections with bacteria. May have some immunosuppressive effect. Has the same problem of lengthening the QT interval and causing sudden cardiac death. Don’t.
Remdisivir
Works by inhibiting the enzyme that allows a virus to do its thing and attach to cellular DNA. Developed originally for Ebola. Shows really good promise in very early studies. Trials happening now. Once safe dosing worked out, will need to scale up production. Promising.
Ritonivir and Lopinavir
Ant-virals devloped for AIDS. Doesn’t work at all.
Immune System Inhibitors
Mainly IL-6 or Interleukin 6.
Trials ongoing and shows some promise. Hard to get but very promising.
Convalescent Plasma
Being given now, has to be obtained from blood of those who had disease.
Shows Promise.
Bottom Line
Until a vaccine comes along, a combination of medications may be effective, but as of now There are NO CURES and precious little in the way of treatment.
Reference:
Here’s What We Know about the Most Touted Drugs Tested for COVID-19: Scientific American Medicine 2020 by Tanya Lewis
It isn’t like there were fewer patients who were sick on my service, in fact there were close to a record number.
But it felt different.
It didn’t feel like we were being overrun, like we would drown in a sea of Covid patients. There were a lot of them, old folks coming in and quickly dying, younger folks coming in and lingering with fevers and shortness of breath, and younger people – wide eyed and frightened as we walked around them in hazmat suits and unavoidably stand away from them as they cough and puff for air praying they wouldn’t end up like that guy over there on a ventilator.
I think it has to do with knowing what to do, what to expect. Sure, we’re making it up as we go along, but hell, so is Fauci and the NIH. it’s just that we’re doing pure battle against a foe that we now know a little about, we see some patterns emerging and feel we have some idea how the bastard operates.
We are all still scared out of our minds, but we have a plan and as long as you have a plan you can do anything.
Morale is surprisingly good on the inside. Where a year ago, there was education done to “teach everyone to be nice”, the staff bends over backwards to be kind, informative, and loving to patients and their families. The families, in turn, are the most grateful I’ve seen in over thirty years. Where in the past no one acknowledged each other in the halls or pretended to look at their phones, we’re all looking into each other’s eyes (all we can see with the masks on) as we pass each other in the halls, saying each other’s names aloud almost like an acknowledgment that we are still together, still ok, still alive.
I will praise our Hospital Administration (not something that folks often do), as throughout this catastrophe they have been transparent , communicative, and responsive. Most of all, they were THERE with us. It is easier to forgive silly oversights when we all realize that we are all just trying to get something right that has never needed to be done before.
Finally for today, I want to thank Chris Brennan MD for gifting me a Tyvex “bunny suit”. Our team (Palliative Care) usually spends enormous amounts of time with our patients, holding hands, talking, and being present to them In this time of patient and staff isolation families ask us to be with their dying relatives, but we can’t. There are only four of us for the whole hospital and that would mean long term exposure to Covid patients with only the barest minimum PPE. So we use what PPE we have and run in and run out. This suit will allow me to sit with our sickest patients and witness their struggles with them. Thanks Chris.
It’s now over a month into the New World and I realize that I’ve only been on the outside six days. I go into the hospital, do my thing, then come home.
The evenings are lost to me as I go through “stages” ( as my daughter has observed). I go from obsessively washing and disinfecting everything I come into contact with, to staring at dinner, to walking around the house looking out of the windows, and finally staring blankly at TV until I lay in bed and stare at my phone in the dark, trying to avoid doing research on Covid (and usually failing) until I pass out.
So it’s safe to say that I’ve only been on the “outside” for 6 days. Just enough time on the weekends to begin to forget what it’s like inside.
This makes reentry difficult.
On the first day back, muscles are tight beyond all as my body tenses in an involuntary cramp all day, the soreness as I relax interpreted to surely be Covid. Any cough from allergies are also Covid, as is the panic when you are too cold or too hot… Covid Covid Covid.
Finally, there’s the ritual of the twice a day temperature checks, the fear as you wait with the stupid thing in your mouth waiting for it to beep… and give you a reprieve for another twelve hours. Another chance to update the instructions in that pended email I have ready to send to my family in case I get sick, one more time.
I think… everyone inside ( on the frontlines or however you want to say it ) feels a similar existential fear.
As far as what it’s like inside :
– Everyone is tired. Maybe not the fatigue of staying up all night, but the dull blankness in the eyes that only lights up when gearing up to go into a room. The fog that only abates when trying to save that life.
– Everyone knows a horror story. A patient whose family won’t give a DNR on an obvious lost cause because three other family members have just died, of the daughter who now lies in the same bed with Covid as her mother who just died of it last night, or of the entire grandparent generation of a family who died on your unit this week.
– Everyone is getting fat. We’re all eating too much, drinking too much coffee, and ignoring ourselves. Maybe if this goes on for another month we’ll all flip to being health nuts, but health food stores don’t deliver to the hospital (for now anyway).
– We’re not crying. I can make that observation but can’t really dissect it, because I’m not crying either.
– In our hearts, we don’t think this will ever be over and for some of us, when it is… it will never be.
A good friend of mine posted on Facebook today (you know who you are), about how there are going to be many cases of PTSD when this is all over. That off-hand observation had me thinking all day long as I donned PPE, saw patients, removed PPE, cloroxed everything around me, and spoke to my colleagues on the “inside”.
Anxiety that burns.
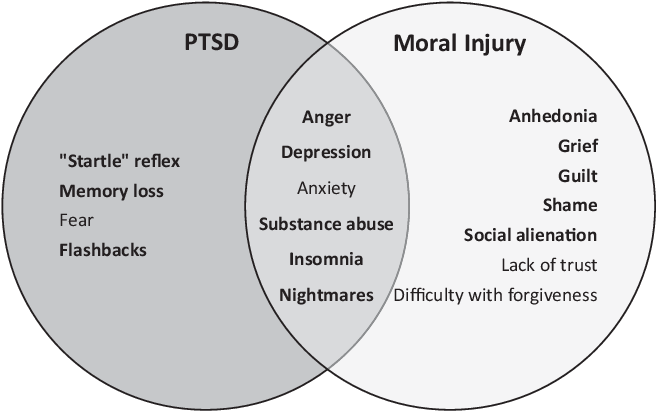
PTSD (Post Traumatic Stress Disorder) is defined by the Mayo Clinic as “a mental health condition that’s triggered by a terrifying event — either experiencing it or witnessing it. Symptoms may include flashbacks, nightmares and severe anxiety, as well as uncontrollable thoughts about the event.”
Moral Injury is defined by the Syracuse University Moral Injury Project as “disruption in an individual’s confidence and expectations about one’s own or others’ motivation or capacity to behave in a just and ethical manner”.
This Pandemic is an ongoing terrifying event for those of us on the “inside”. We see and experience things that on a normal day would horrify any reasonable health worker and we shrug it off with “I’m good”, spray Virex (carcinogenic by the way) over our one -gown-a-day, and move on.
Much like in war, we are suffering Moral injury as well. The things we tolerate, the actions we take for the “greater good”, and the small acts we do to let us know we are still human are causing damage on a daily basis.
We strip outside and wash everything before setting foot at home, we don’t hug anyone anymore (loss of human contact), we obsessively disinfect everything… and death becomes just another thing, something in which you cannot invest.
PTSD vs Moral Injury
Much like in war, this is not going to be over for years. When the media has moved on to the next shiny object, Health Care Workers will still see the horrors of random deaths by suffocation and kidney failure as a normal thing. We’ll still be wearing masks, shoving gloves in our pockets, and having a severe mistrust of human touch.
So yeah, “when this is over” there will be a lot of us who will leave the field, and a lot of us who won’t, but will be forever scarred and will carry the burden that our military now carries of Anger, Depression, Anxiety, Substance abuse, Insomnia, and Nightmares. I hope we will learn, because the Medical Community is much worse than any other in taking care of itself, I fear we won’t.
If not, we’ll see the same incredible suicide rate that we see in our military among those of us who “gear up and go in” on the “inside”.
I hope we’ll be able to care for ourselves as bravely as we care for others.
It has been my experience, that when you are tired (I mean tired to the soul), memories are imprinted in a series of “snapshots” that expand into full movies, kind of like thumbnails of movies on YouTube.
A little tired.
This was the case today.
I have the privilege of working all over the hospital, not just with “my people”, but going from ER to the OR and everywhere in-between. So I see so many things that they “store “ as snapshots or moments in time that I can touch and replay at will ( and sometimes they replay against my will). I’ll share some of them with you.
– The barely controlled frenetic energy of the emergency room, hazmat suited doctors and nurses contrasting with the aides trying to choose a good food tray for that “patient in 8 who is really hungry”.
– The zush zush zush sound of the nurses and aides as they walk through the halls in their tyvek “bunny suits“ going from room to room taking care of the dying and the not dying yet.
– The eerie subdued lighting and oppressive quiet of what was once a holding room for elective procedures that is now a “fishbowl” of Covid patients all in a circle. Those of us working inside quietly desperate as we can almost “feel” the virus in the air.
– The frightened look in the eyes of the nurse caring for the Covid patient in the recovery room isolation area, her unseen smile and insouciant attitude covering up her fear.
– Half heard conversations on the new temporary ICUs among nurses who have never met before, declaring bravely that “we’re the cool kids now” as they gear up.
– And finally the seemingly endless phone calls I made to Spanish speaking families (I’m native born Spanish speaker in case you didn’t know) about how their Mom/Dad/Son/Daughter/Grandmother/Grandfather is NOT going to get better and that yes, I will pray with them.
Hey, stay safe, get some rest, so we can do it again tomorrow.
Since this has all started there have been several waves here in the hospital.
First there were the old nursing home patients, then there are the younger folks with co-morbidity.
Now we are seeing the lower socioeconomic community, the Hispanic and African American community. I work in a fairly well off Hospital in a fairly well of suburb of New York, but there has always been this “service” class that has existed if not unofficially, certainly not counted in the minds of those who plan for these things.
This will change in the future I hope as the second wave of COVID is exposing the system for never seeing them.
On the bright side, we are discharging many more people safely to home and every time someone who has survived Covid goes home they play “Here comes the sun” overhead. It makes you smile to know not all is about death.
The next weeks are a marathon as we keep sweeping against the tide. We can only hope to have enough left in our own tanks to get us through.