So the “inside” is looking a lot less like the “inside” every day.
When I resumed these posts, It was at the run-up to the surge in New York (Long Island more specifically) and I watched an orthopedic floor turned into an ICU, I saw nice clean step-down beds (were people go to have some cardiac monitoring – but nothing too “serious”) turned into ICU beds, a holding room for elective surgeries turned into “the fishbowl” of Covid patients were patients watched each other suffocate, and even ambulatory surgery units turned into Covid – care floors.
Like the receeding tide, I am seeing units being returned to their former functions, being made “clean” again. More and more, we are allowing families to at least come and see their sickest relatives before they are necessarily near death. We are even going to open a new cafeteria expansion next week (3 months late because of Covid).
There is a sort of strange melancholy to this process, as the huge bags of “dirty” supplies get thrown out and the rooms are “terminally cleaned” it feels like the day after christmas, after the superbowl, after the world series… the world returning to whatever passed for normal, the exploits and adventures spoken only in “remember whens”.
I look at the sparkling clean rooms and still see the hundreds of patients who suffered and died in them and I don’t want them to be forgotten, their suffering should not have been in vain.
And then I see the crowds rushing to bars and swimming pools and such flouting common-sense self protections and think, “yeah they did die in vain, and it is going to happen again, somewhere else if not here”.
I want it to be over.
I am afraid it is not.
As Always
Wash your hands
Don’t touch your face
Wear a mask… you aren’t freaking superman / captain marvel.
Exercise, eat right.
Love one another, hate doesn’t make anyone better.
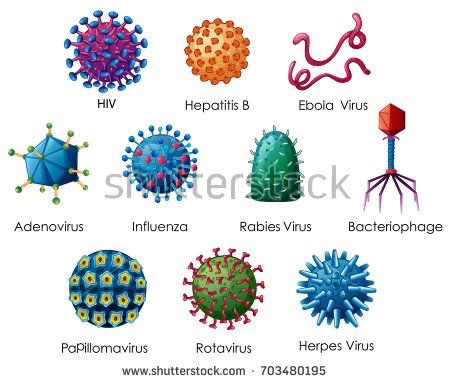
Viruses are small, very small. The reason they can be small like that, is that they aren’t burdened with the need to have structures that real live organisms need to qualify them as being alive.
To recap, viruses are tiny bits of genetic material surrounded by a shell and an injector mechanism. It has no way to generate energy, it can’t eat, reproduce on its own, or move on its own.
So considering that viruses don’t need all those bells and whistles, they can be small.
Viruses don’t fly
Since viruses are small, and have no structures that make them alive, they also don’t have wings, jet engines, wheels, or any other way to get around on their own.
In order for a virus to be spread, it needs a “vector “ (a means of transfer). It can be fecal-oral (yeah, exactly what it sounds like) like hepatitis A is spread (ewww), fomites (surfaces), or in aerosol droplets. Aerosol droplets are small, but are huge in comparison to a virus particle.
Considering this virus needs to enter through the mucus membranes of the upper respiratory tract, it’s got to get from the mouth or nose of one person to another.
Touching something that has live virus on it then touching your mouth/nose/ or face is a good way to get it, therefore the warning to wash your hands.
But think about it, how do these viruses get on the surfaces, rarely do people lick counter tops or doorknobs (this isn’t that kind of blog) the most likely culprit is aerosols landing on these surfaces.
Remember, viruses need a helper. When a person coughs, a huge number of mucus particles that necessarily contain a wide sampling of all your mouth flora spew into the air (about 6-8 ft). That’s why the social distance recommendation is made.
Mask
So the main reason for the mask, is to keep your particles from blowing all over creation and to prevent other people’s gross little virus bombs from getting on your mucus membranes.
An extra benefit is that it’s hard to touch your mouth and nose while wearing the mask.
So although technically, most masks cannot stop a free flying guided missile version of a virus, the mask doesn’t have to!
It only needs to decrease the number of relatively large particles from one mouth to the next.
Masks work.
This has been the basis of why surgeons use masks and wash their hands for over a hundred years. And it DOES WORK.
Wear the mask, don’t be a statistic, the best revenge is to live well and stay healthy.
It’sBeginning To Change
The “inside” isn’t so inside anymore. With fewer admissions for COVID, the hospital is clearing and cleaning entire units in preparation to begin regular operation (at least somewhat). It’s wonderful… and yet.
The closeness that developed between people who had never met before will slowly become a memory, the usual Balkanization of Hospital life returning to pit us all against each other for attention (and the accompanying allocation of resources).
I hope that the sense of unity and the camaraderie we had during this time of “combat” remains and we don’t forget what it meant to heroes to each other as well as to the patients.
There is a strong possibility that we’ll be called upon to do it again…
Medical update
Sadly, not much that we have in the armamentarium works in the way we give it now. The drugs we need to try (in combinations and earlier) are NOT generally available. From anywhere!
Vaccines (despite happy talk on TV) are NOT right around the corner. Antibodies are still not known for sure to give immunity. In short, we are STILL working with No Ammo.
The only things we can do right now is wear masks, social distance, wash hands, exercise, eat healthy, and LOVE ONE ANOTHER.
Please do not take chances and become a statistic. Go out into the world again armed with as much knowledge and common sense as you can. It seems to be in short supply.
Being smart and prepared is NOT a sign of weakness, flouting common sense is.
1. A brand new 3M N-95 mask smells a little like vanilla ice cream.
2. All nurses are amazing.
3. You can’t shock an ER nurse.
4. ICU nurses will save your life.
5. Nurses who have ever cared for COVID patients are certified Badass, will chew steel for lunch and spit out nails.
6. I would go into battle with any nurse at my side.
6a. Nurses Aides are the infantry in healthcare, they do the grunt work and come up with most brilliant observations in the fight. The view that is often overlooked by the higher ups.
7. There is a whole population of younger people (35-60 yo) who’ve contracted COVID who are alive, on high flow and high percentage oxygen, can’t move more than side to side, and are trapped as chronic pulmonary disease patients likely forever.
8. There is a whole new population of younger people (35-60 yo) who’ve contracted COVID who are now on hemodialysis as well as chronic pulmonary disease patients.
9. The medical system will have to re-create the “sanatorium” system for these patients for many years to come to aggregate these patients under the care of expert Doctors and Nurses if they are to have any hope of return to society.
10. Most of what we give now (in terms of medications) and the way we give it now is minimally effective.
11. The best treatments are oxygen, prone positioning, nutrition, great nursing care, and love.
12. It is genuinely frightening to walk into a building every day knowing that you could get a deadly disease, pass it to everyone you know, and become just another statistic, a mere number in a ledger.
13. It is frightening to realize that this is going to be the way it is for a VERY long time (even when there is a vaccine).
14. Much the same way that “every Marine is a rifleman first”. Every physician should be capable of intelligently and effectively managing a patient from top to bottom, specialty comes later. This should be reviewed on a certain timetable, not by testing, but by doing.
As always, wash your hands, don’t touch your face, wear masks in public, do the social distance thing, and practice love and kindness. There is too much hatred in the world.
It is rare and NOT widespread, this post is for informational purposes only.
In the last week there has been the identification of a pediatric syndrome that seems to be associated with Covid 19 infections in children.
It appears to be an inflammatory reaction by the body to the Covid virus. As we’ve discussed in previous posts, in adults a good bit of the damage appears to come from the body’s immune system attempting to eradicate the virus without the proper tools (antibodies) and just lobbing non-specific inflammatory “bombs” everywhere.
Unfortunately, this looks to be a similar thing but accelerated. It is still early and the condition is still not fully understood, but I’m putting out the information on Pediatric Multi-system Inflammatory Syndrome from NYC Health and Hospital Corp. for your consideration.
As always, please wash hands, don’t touch face, social distance and wear masks in public. Please follow the advice of the local heath departments and the CDC.
They really care about your health and the health of your children
Fact Sheet: Pediatric Multisystem Inflammatory Syndrome What is pediatric multisystem inflammatory syndrome? Pediatric multi-system inflammatory syndrome (PMIS) is a new health condition appearing in children in New York City (NYC) and elsewhere. Some doctors think the condition is related to having coronavirus disease 2019 (COVID-19), but the connection is still not clear. PMIS is like other serious inflammatory conditions such as Kawasaki disease and toxic shock syndrome. Children with PMIS can have problems with their heart and other organs and need to stay in a hospital to receive support in an intensive care unit. PMIS is a rare condition. However, because it is life-threatening, it is important that parents know the signs and symptoms, so they can get help right away. What are the signs or symptoms of PMIS? Most children have fever (temperature of 100.4 degrees F or 38.0 degrees C or greater) lasting several days, along with other symptoms. Common symptoms include: • Irritability or sluggishness • • Abdominal pain without another explanation • Diarrhea • • Vomiting • Rash • • Conjunctivitis, or red or pink eyes When should I call my child’s doctor or get emergency care? You should call your doctor immediately if your child becomes ill and about any signs or symptoms your child has and use that information to recommend next steps. If your child is severely ill, you should go to the nearest emergency room or call 911 immediately. Is PMIS contagious? PMIS is not contagious, but it is possible that your child has COVID-19 or another infection that may be contagious. This is why hospitals will take infection control measures when treating your child. Is there a treatment for PMIS? Currently, children with PMIS are being treated with different therapies, including intravenous immunoglobulin and steroids. These drugs help reduce the body’s immune response that causes the inflammatory syndrome. Children are also being given other medications to protect their heart, kidneys and other organs. How can I prevent my child from getting PMIS? Although we do not know yet if PMIS is related to COVID-19, you should still take steps to prevent your child from being exposed to COVID-19. Face coverings, hand hygiene, and physical distancing are the best way to prevent COVID-19. Children with underlying medical conditions can be at higher risk for poor outcomes of COVID-19, so you should make sure they follow COVID-19 prevention measures. The NYC Health Department may change recommendations as the situation evolves.
“Perseverence is the hard work you do after you get tired of doing the hard work you already did…“**
Covid – 19 in May 2020
There’s an old expression that people use when describing the attempt to bring change to an organization or group while not disrupting the function of the group, “it’s like building a plane while its in the air”.
Yeah, it’s on fire.
In the case of the medical response (we’ll not even get into the national political response) to the COVID – 19 pandemic, we’re trying to build the airplane while its in the air… and its on fire too.
Unfortunately, the medical response has initially been mixed in with the politics and considering that we had nothing to treat this disease at the begining, didn’t harm the response as much as merely confuse the hell out of the general public.
Let’s get to it
To work
What I will do in this post is to review the latest on the drug therapies that we have available and I will separate what is fact-based vs what is my opinion based on what I know and extrapolations.
Hydroxychloroquine
The initial hoopla about this drug comes from early Chinese reports. There were also some communications from France and Italy in which they claimed that there was some decrease in the viral load in the sputum (mucus, spit, phlegm) of people who were given this drug. Why did you give a drug that has no anti-viral properties to these patients? Did the lower viral load improve symptoms? Did the lower viral load improve survival?
The answers (after someone collated and finally looked at the reults) were that 1) they didn’t exactly know why they did it, 2) they were very few of them anyway, 3) the decreased viral load wasn’t significantly (statistically) decreased, and 4) it didn’t seem to improve symptoms nor survival.
So bottom line, it doesn’t work (it never did), it has horrible side effects (including death), and it is a complete waste of time.
Azithromicin
Essentially the innocent bystander in this whole thing, it was used as an adjunct (can something that doesn’t work be used to help another thing that doesn’t work?) to Hydroxychloroquine in the early trial and error phase of Covid treatment. It has an unfortunate side effect of altering the EKG which is usually not a problem as it is given for five days only and usually in relatively healthy people, but in sick patients taking Hydroxychloroquine it was a potentially lethal combination.
Bottom line, it’s good for sinusitis and mild bacterial infection but not COVID.
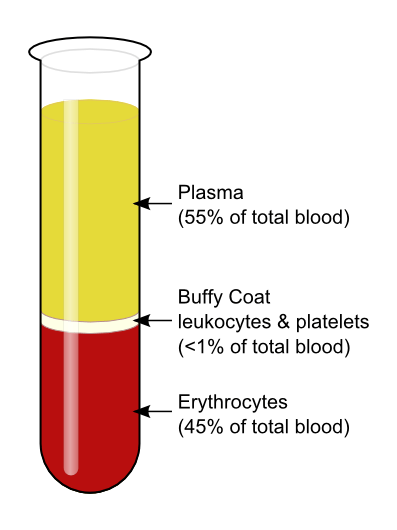
Convalescent Plasma
This is an old stand-by of treating a viral type disease that dates back to 1883 when the different components of blood were discovered. The theory goes back even further to the idea of animism, in that the blood of a survivor must have in it the makings of a survivor.
In a more up-to-date sense, we know this to be true as the person who survives a serious infectious disease does indeed make antibodies to that infectious agent. What we don’t know is if these antibodies will shorten the disease, improve symptoms, or improve survival.
It is being given to severely ill patient’s in hospitals. It is intravenous. Plasma is also very tightly controlled and only given by strict criteria. The reason for this is that the blood plasma has many other components such as coagulation factors and such that could in and of themselves be dangerous. It may also be possible to cause allergic reactions in the recipient.
Bottom Line: It is being given. We don’t know when is best, we don’t know the optimal dosage, and we don’t know if it is doing any good. (Opinion: I wish I could say that I saw great improvement in these severely ill patients, but I haven’t). We remain hopeful that this will be an important part of treatment for now. More data to come.
Remdisivir
Self explanatory
Originally developed as a broad spectrum (general purpose) anti-viral for Ebola, this drug interferes in the reproduction of the viral mRNA (the chemical that produces more virus) by messing with the mechanisms that hijack the reproducive mechanisms of the host cells. It is not a cure, but it does slow down the replication of the virus, which in turn preserves more of the body’s own native cells, presumably giving the body time to make antibodies.
Bottom Line: It is still strictly controlled. It is intravenous. Since we aren’t really sure when to give it, and how much, we are still sticking to the study criteria that the manufacturers have laid out. In my opinion, this drug would be most useful when given very early in the illness when the virus is first making it’s attack on the body through the lungs. As it is, we don’t have enough drug (as of this writing, there are close to 1.5 million known cases of COVID – 19 in the US alone and if given more than once -protocols are now for twice daily for 5 days – that would be 15 million doses that would be needed tomorrow) to begin to give it to everyone who will eventually need it.
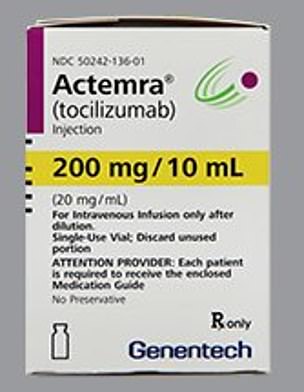
Actemra (Tocilizumab)
Fun Fact: if it ends in a -ab it’s IV, in a -ib it’s a pill
Actemra is a member of the class of drugs called a “biologic”. This is used mainly for people with severe arthritis and it comes with it’s own set of side effects which come from its main function as an immune modulator. What this thing does is to block one of the inflammatory chemicals (The “hand grenades” from an earlier post, called IL-6).
Since the really destructive part of the body’s destructive reaction to COVID – 19 is it’s uncontrolled inflammatory response, a drug that can “diffuse the hand grenades” and blunt the out-of-control inflammatory response would help enormously.
The problem is that there are no studies out yet that use this drug in any numbers that would give us good information on how best to give it and for how long.
Bottom Line: We are giving it in the hospitals. It is IV. It is severely in short supply. I have seen some very good anecdotal (personal experience) responses to this.
Synthesis (Opinion)
From here on in I am giving my opinion on treatment. I believe that we must use a multi-pronged approach to this COVID – 19 constellation of symptoms based on how this disease manifests in humans.
When the virus begins attacking the lungs, a Remdisivir type drug should be started to limit the attacking invader. An Actemra type drug should then be used to dampen the massive inflammatory response of the body that causes the actual damage to the tussues (especially distant damage) and then plasma might be useful as an adjucnt to the initial therapy.
Only by using all the tools available to us will be able to temporize and buy time and save lives until a vaccine is created that will help us land the plane (that was on fire) safely.
In future posts I will discuss any changes to the above indications or medications as they come in and out of favor but I won’t rehash any of the older information. Unfortunately, this virus looks to be sticking around for awhile and I don’t want you to get bored.
As always
Wash your hands. Don’t touch your face. Exercise. Eat right. Social distance. Wear a mask in public. Be kind and be patient.
The opinions expressed here are mine and do not reflect the opinions of any medical organization.
In the last week or so, the pace of life on the “inside” has been marked by a steady change in how the world works for us.
Early on, it was preparing for the surge, then it became the overwhelming fear and frustration as we were seemingly swallowed by the onslaught. However, over the last week it’s different. We seem to be settling in for the long haul. Its NOT going to be over soon. We’ll push it to certain areas of the hospital, but it is not going away.
In an earlier post, I’d said that we seemed to be getting a handle on it… it was naive of me to say that. We had discovered the rhythm and the pattern of the illnesses but not exactly how to beat it.
The Virus
Paths of Disease
The asymptomatic (no symptoms) form is as if you had nothing, maybe a little sniffle at most. You get better on your own but hell… you didn’t know you had it. You remain infectious.
The mild form is the at home version that you hear about… Chris Cuomo on CNN and such. It looked awful, and it is, but the fevers and shortness of breath are survivable.
There’s the moderate reaction to the virus which is like the mild form but with the extra added attraction of hypoxemia (low blood oxygen) and shortness of breath that often leads people to come to the ER. These folks are usually admitted, given oxygen, vitamins, whatever the cocktail (of medications and vitamins) of the day, made to lay down on their bellies (the prone position) and watched to see if they get better or not.
From there it splits:
1) You get better and are sent home on oxygen to recover.
2) It Gets Worse.
If you get better, you get better. If it gets worse you go one of two ways (generally):
The Long Slow Burn:
You cough and get low blood oxygen. Over time the lung damage causes you to need higher doses of oxygen. The lucky ones eventually heal and are weaned off the oxygen. If you are not lucky, you get stuck at this level. There are many people stuck in the hospital at this level.
The Long Blaze:
Your lungs can’t supply the body with oxygen and you get intubated and put on a ventilator. This can be for a long time. Since this whole deal has only been going on for around two months we don’t know how long, but the longer you are on a ventilator, the worse it is. There are many people who come off so there is hope, its getting better the more experience we get.
Anticoagulation
So there is talk online about Covid – 19 causing abnormal blood clotting and people taking blood thinners. Whenever someone is seriously ill, there is a chance of blood clots. This bugger has a chemical that causes the clotting system to go haywire in its envelope, so during critical illness there are blood thinners used. DO NOT TAKE BLOOD THINNERS TO PREVENT COVID – 19.
Medications
Hydroxychloroquine (Plaquanil) – NO
Zithromax – Not for Covid
Zinc – 50 mg of elemental Zinc for maximum of 12 weeks max
Vitamin C – Maximum of 2,000 mg a day
We’re Getting there
Multivitamins – Sure why not?
Plasma – plasma from people who have had the disease. We don’t know dosages and we don’t know if it works.
We are giving it in hospital only.
Remdisivir – Developed for Ebola and has been shown to decrease time of active disease. It is only IV and we don’t yet have the actual correct dosages yet.
But this is actually looking good.
Bottom Line
– Wash your hands
– Wear a mask in public
– Practice Social Distancing
-Exercise
-Stop Smoking
-Eat Right
-Stay Away from stuff that can stress you out (I’m looking at you News and Facebook).